Liver Cancer, primarily hepatocellular carcinoma (HCC), ranks as the most common primary malignancy of the liver and a leading cause of cancer-related deaths worldwide. Early and accurate diagnosis is crucial for improving prognosis, as survival rates drop significantly with advanced stages. Diagnostics involve a multimodal approach combining clinical evaluation, laboratory tests, imaging, and histopathological confirmation.
Risk factors such as chronic hepatitis B/C, cirrhosis, alcohol abuse, and non-alcoholic fatty liver disease guide surveillance in high-risk populations. Guidelines from organizations like the American Association for the Study of Liver Diseases (AASLD) and European Association for the Study of the Liver (EASL) emphasize non-invasive imaging for diagnosis in at-risk patients, often avoiding biopsy.
A typical diagnostic algorithm for suspected HCC.
Another flowchart outlining surveillance and diagnostic steps for HCC.
Clinical Evaluation and Risk Assessment
Diagnosis begins with history, physical exam, and risk stratification. Symptoms like abdominal pain, weight loss, or jaundice often appear late. High-risk groups (cirrhosis, chronic viral hepatitis) undergo regular surveillance with ultrasound and serum alpha-fetoprotein (AFP) every 6 months.
Laboratory Tests: Tumor Markers
Blood tests play a supportive role.
- Alpha-Fetoprotein (AFP): The most widely used marker; elevated levels (>20 ng/mL) suggest HCC, though not specific (also raised in benign conditions). Highly elevated (>400 ng/mL) in context can be diagnostic.
Illustration of AFP blood test in liver cancer screening.
Another depiction of AFP testing for HCC detection.
Other markers include des-gamma-carboxy prothrombin (DCP/PIVKA-II) and lectin-bound AFP (AFP-L3), used in combination for better specificity.
Imaging Modalities
Imaging is cornerstone, especially contrast-enhanced multiphase studies.
Ultrasound
First-line for surveillance; cost-effective and non-invasive. Detects nodules but lacks specificity for characterization.
Ultrasound image showing a liver tumor.
Procedure and example of liver cancer ultrasound.
Secondary liver cancer on ultrasound scan.
Computed Tomography (CT)
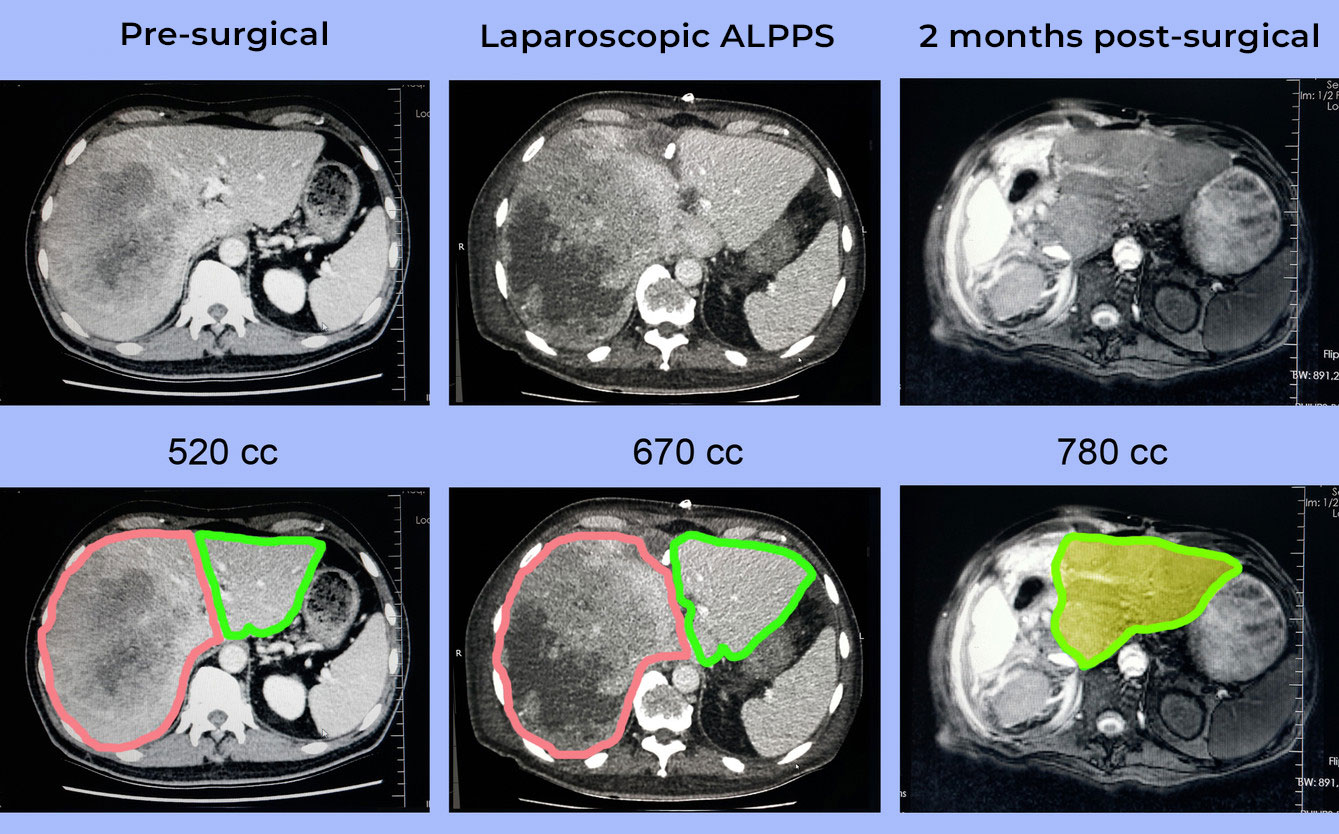
Multiphase CT (arterial, portal venous, delayed phases) shows classic HCC enhancement: hypervascular in arterial phase, washout in venous/delayed.
CT scan comparing normal liver to HCC.
Contrast-enhanced CT highlighting liver cancer.
High-resolution CT of liver tumor.
Magnetic Resonance Imaging (MRI)
Superior soft tissue contrast; preferred for equivocal cases. Uses gadolinium contrast; HCC shows similar arterial enhancement and washout.
MRI scan of liver with HCC features.
Multiphase MRI sequences for HCC diagnosis.
Contrast-enhanced MRI illustrating liver cancer survival predictors.
LI-RADS System
The Liver Imaging Reporting and Data System (LI-RADS) standardizes reporting for CT/MRI in at-risk patients, categorizing lesions from LR-1 (benign) to LR-5 (definite HCC).
LI-RADS category overview chart.
Detailed LI-RADS interpretations for HCC.
Histopathological Confirmation: Biopsy
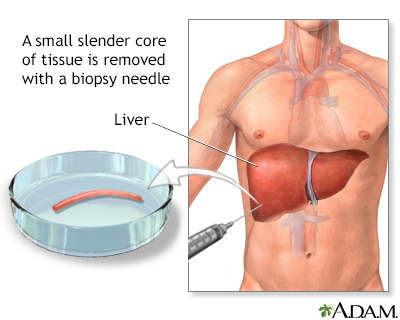
Biopsy is reserved for indeterminate lesions or non-cirrhotic patients. Percutaneous needle biopsy under imaging guidance provides tissue for microscopy.
Illustration of liver biopsy procedure.
Standard depiction of percutaneous liver biopsy.
Pathology slides show trabecular patterns, Mallory bodies, or specific stains (e.g., reticulin loss).
Microscopic view of hepatocellular carcinoma.
H&E stained HCC pathology slide.
Another high-magnification HCC histology.
Emerging Diagnostics
Liquid biopsy (circulating tumor DNA), AI-enhanced imaging, and novel markers like Glypican-3 are advancing early detection.
Challenges and Considerations
False negatives in small tumors, radiation exposure (CT), cost (MRI), and biopsy risks (bleeding, seeding) pose challenges. Differential diagnosis includes metastases, cholangiocarcinoma, and benign lesions like hemangioma.
Conclusion
Liver cancer diagnostics integrate surveillance, biomarkers, advanced imaging, and selective biopsy for timely intervention. Adherence to standardized systems like LI-RADS ensures accuracy, while innovations promise improved non-invasive detection in high-risk populations. Early diagnosis remains key to better outcomes in this aggressive disease.
More articles by ZMR Researche:
https://www.zionmarketresearch.com/de/report/cardiovascular-monitoring-diagnostic-devices-market
https://www.zionmarketresearch.com/de/report/aluminum-forging-market
https://www.zionmarketresearch.com/de/report/wavefront-sensor-market-size
https://www.zionmarketresearch.com/de/report/lip-augmentation-market